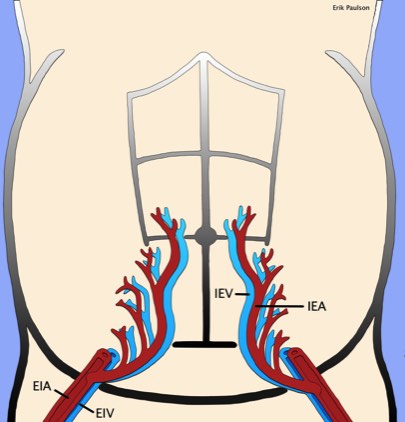
Check with ultrasound to make sure there is an adequate window to drain the fluid. Make sure to find the inferior epigastric artery with Doppler in order to avoid it. Typically, the best window will be in the right or left lower quadrants just lateral to the inferior epigastric arteries (see diagram below).
Mark the area where your needle will enter the skin.
Consent the patient, making sure to discuss major risks of bleeding, infection and bowel perforation.
Open the tray and put on sterile gloves.
Draw up the lidocaine into the syringe (typically 10 cc is adequate) and attach a 25 gauge 1.5 inch needle.
Use iodine or a Chloraprep to sterilize the region you previously marked.
Cover the surrounding areas with a drape or sterile towels.
Place a sterile probe cover over the ultrasound probe. The probe cover is optional but recommended if the volume of ascites is low or moderate. Using constant ultrasound guidance will help to avoid puncturing a segment of bowel in these cases. I personally like the linear probes but a small curved probe will work as well.
Insert the 25 gauge needle with lidocaine into the subcutaneous tissue (shallow) and make a raised wheal in the area you marked previously. This should not take more than 2 cc of lidocaine.
Now, with ultrasound guidance, insert the 25 gauge needle through the wheal all the way to the peritoneal lining. Inject a couple cc onto the peritoneum and then inject the rest of the lidocaine as you pull the needle out.
Make a 0.5 cm dermatotomy.
Under continuous ultrasound guidance, insert a 5 French Yueh centesis catheter through the dermatotomy, the subcutaneous tissue, the peritoneum and into the fluid being careful to avoid bowel.
When fluid returns, hold the inner cannula of the Yueh centesis catheter in place while you advance the outer catheter.
Attach the catheter to plastic tubing and have the technician connect the tubing to a vacuum suction container or a wall vacuum.
When the fluid stops draining, check with ultrasound to make sure it has been mostly removed. Sometimes, because of the suction, the tip of the catheter will stick to a segment of bowel and stop draining. This can be solved by clamping the plastic tubing (to release the suction) and twisting or slightly retracting the Yueh centesis catheter.
Remove the Yueh centesis catheter and place a bandage or pressure dressing (if leaking).
Send the fluid for diagnostic studies, if indicated.


{kind=link}